Solving the Texas Health Care Shortage
By Dr. George Mills, Regional Chief Medical Officer for Oklahoma and Texas and a VP of Physician Services
Texas, like most U.S. states, is experiencing a clinician shortage that continues to exacerbate. For context, on a scale from 1 to 50, where 1 is the highest ratio of physicians per 100,000 people, the Association of American Medical Colleges ranks Texas 42nd of the U.S. states for physician shortage across all specialties. By 2032, Texas is projected to be short 10,330 physicians and 12,570 vocational nurses. What can be done?
While this poor ranking is no doubt multifactorial, it stems from several key causes: an aging population, the rapid growth of Texan business and state populations, and decreased funding for medical education. Additionally, hospitals have attempted to mitigate declining reimbursements with more service offerings, further magnifying the clinician shortage.
As NorthStar Anesthesia’s Regional Chief Medical Officer in Oklahoma and Texas, I am acutely aware of the impact a shortage of anesthesiologists and CRNAs (Certified Registered Nurse Anesthetists), is having on the Texas community.
For context, in 2022, 2,000 anesthesiologists and 2,200 CRNAS graduated or entered the workforce, 2 – while 7,000 anesthesiologists and CRNAs left the workforce. Meanwhile, an anesthesia employment site indicates that there are thousands of job openings for CRNAs – with 542 being in Texas alone.
This trend, affecting the entire health care industry, has resulted in backed-up ERs, delayed surgeries, and burnt-out clinicians, undoubtedly impacting patient care. Furthermore, as the limited quantity of clinicians are stretched thin, clinicians demand higher compensation. Due to decreased payments from CMS and commercial payers, much of the provider compensation expenses are ultimately passed on to our hospitals.
However, I believe there are several actions we as health care professionals can employ to strengthen the clinician pipeline and reduce the staffing shortage.
First, we must increase the number of graduate medical education (GME) programs and residency spots. For context, to become a practicing, licensed U.S. physician, candidates must complete an accredited graduate medical education (GME) program, which includes residencies. However, the 1997 Balanced Budget Act (BBA) set a cap on how many GME residents and fellows Medicare would support.
It is encouraging that Texas lawmakers have appropriated $520.5 million for the state’s GME Expansion Grant Program since 2014, supporting 465 new first-year GME positions. Texas has also launched more than six new medical schools since 2016, and a new university program at TCU has partnered with three health systems to open 260 medical resident positions by 2028. These opportunities should help bolster Texas’ ratio of 1.1 first-year residents to 1 medical graduate, a ratio which Texas has met and maintained since 2018. I believe other states should follow suit.
Meanwhile, by 2025, all new CRNAs will need a doctorate degree, raising the barrier for people to become CRNAs and making it harder for hospitals to recruit qualified CRNAs. Like for GME programs, we should increase funding for CRNA doctorate programs that enable scholarships and entice prospective nurses – as studies estimate that CRNA programs will need to double the number of graduates to meet patient demand in the coming years.
Second, we should make concerted efforts to improve work-life culture for health care providers. We are all aware of the emotional strain our clinicians are under due to the nature of their work – especially after COVID-19. A 2021 Mayo Clinic study found that 62.8% of physicians are experiencing some sort of burnout, and a 2021 American Nurses Association study found 72% of CRNAs experienced at least a moderate level of burnout.
Hospital administrations must implement system-wide solutions to address the excessive workloads and lack of organizational support which lead to burnout and lesser employee retention. In my region, we have fostered leadership development and designed flexible work options to improve culture and provide more clinician support. NorthStar also closely monitors our clinician staffing numbers to ensure professional sustainability. We cannot expect teams to maintain themselves if they work unreasonable hours in increasingly stressful environments.
Finally, we must recruit local physicians to increase retention. Texas DSHS research found that Texas maintains the third-highest U.S. physician retention rates when both medical school and residency training occur in-state. Between 2000 and 2019, 58.9% of physicians who completed graduate medical education in Texas ultimately stayed in the state to practice. Specifically, anesthesiologists who completed graduate medical education in Texas had a 59.3% average likelihood of practicing in Texas. This evidence supports the need to focus recruitment on Texas medical student graduates for our residency programs.
There is no doubt that clinician shortages are an acute problem both in Texas and in anesthesiology. Despite the numbers, I am encouraged by our cross-team creativity and collaboration and incremental progress we’ve made to recruit and retain Texas talent, enabling us to offer industry-leading care. I hope others will recognize that this issue is not unique to Texas and begin investing in recruiting and retaining the best talent to improve patient care.
6255 State Hwy 161 #200
Irving, TX, 75038 USA
214.687.0001
Copyright 2024 NorthStar Anesthesia. All rights reserved.
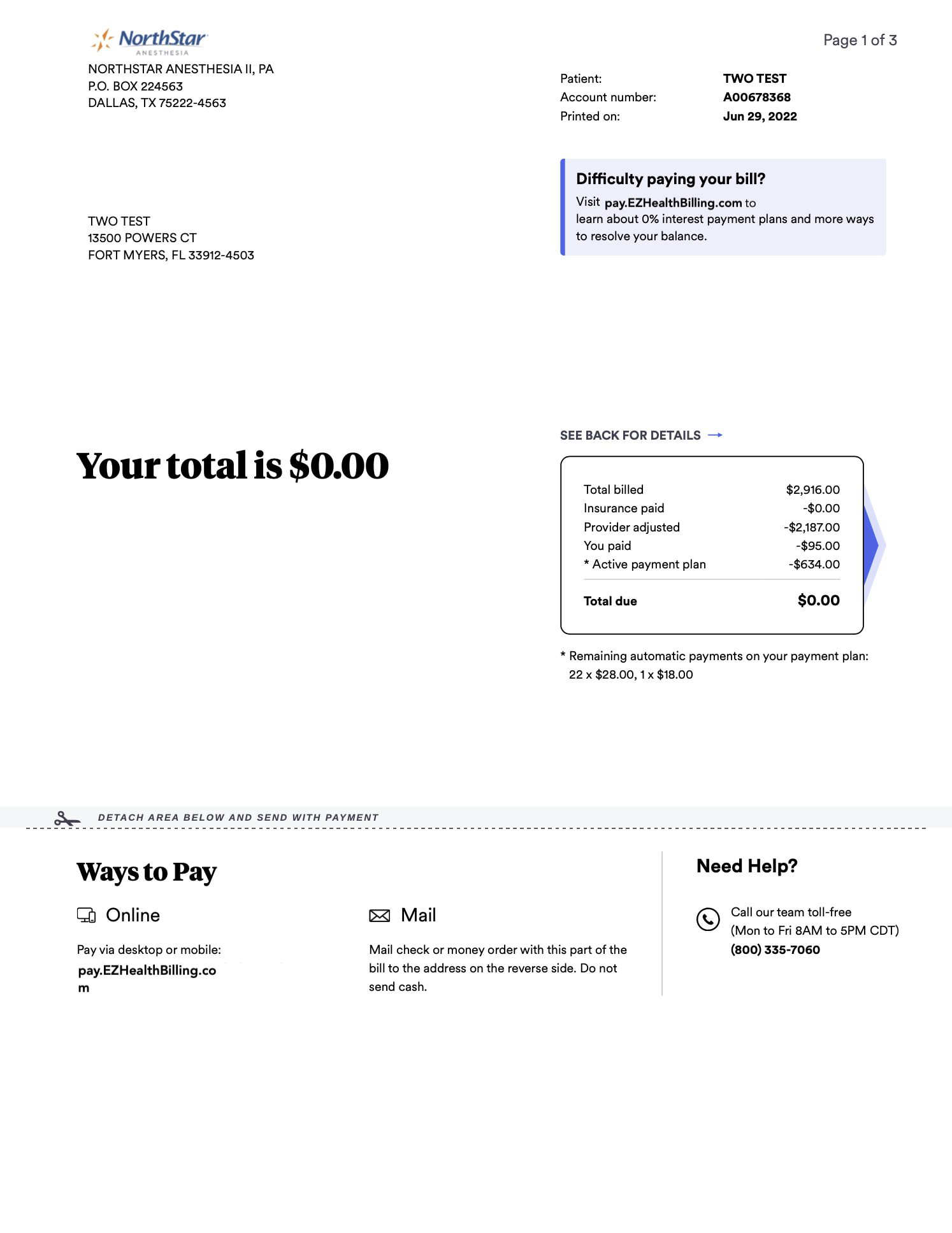
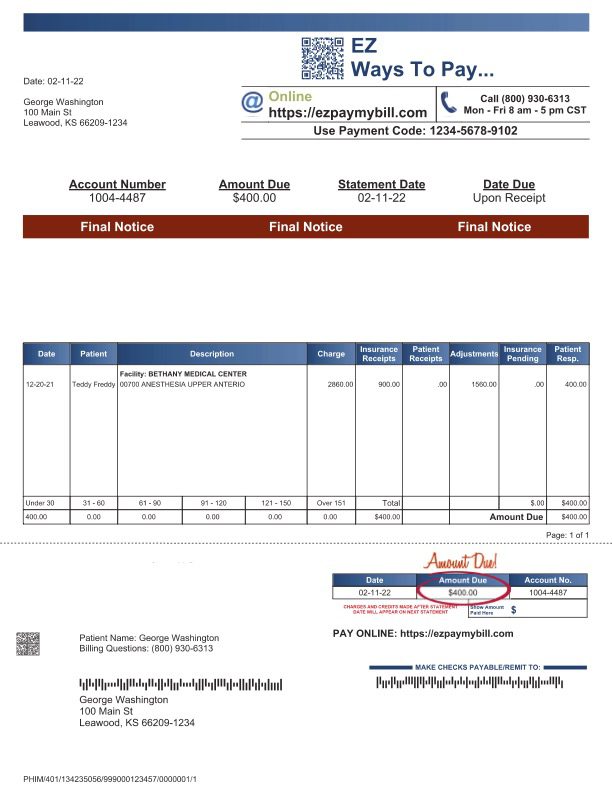
To pay your bill, click on the invoice that looks most similar to your invoice.